You may schedule a confidential appointment in my office to
explain any topics or treatment options discussed on this
page.
Carotid Endarterectomy:
What is It?
A carotid endarterectomy is a surgical procedure in which a doctor removes
fatty deposits from one of the two main arteries in the neck supplying blood to
the brain. Carotid artery problems become more common as people age. The
disease process that causes the buildup of fat and other material on the artery
walls is called atherosclerosis, popularly known as "hardening of the arteries."
The fatty deposit is called plaque, the narrowing of the artery is called
stenosis. The degree of stenosis is usually expressed as a percentage of the
normal diameter of the opening.
Why is the Surgery Performed?
Carotid endarterectomies are performed to prevent stroke. Two large clinical
trials supported by the National Institute of Neurological Disorders and Stroke
(NINDS) have identified specific individuals for whom the surgery is highly
beneficial when performed by surgeons and in institutions that can match the
standards set in those studies. The surgery has been found highly beneficial
for persons who have already had a stroke or experienced the warning signs of a
stroke and have a severe stenosis of 70 percent to 99 percent. In this group,
surgery reduces the estimated 2-year risk of stroke by more than 80 percent,
from greater than 1 in 4 to less than 1 in 10.
In a second trial, the procedure has also been found highly beneficial for
persons who are symptom-free but have a severe stenosis of 60 percent to 99
percent. In this group, the surgery reduces the estimated 5-year risk of stroke
by more than one-half, from about 1 in 10 to less than 1 in 20.
What is a Stroke?
A stroke occurs when brain cells die because of decreased blood flow to the
brain. In some cases, small pieces of plaque in the carotid artery may break
loose and block an artery in the brain. The narrowed opening in the carotid
artery can be a source of blood clots that travel to the brain, can trap blood
clots from other areas of the body, or can become completely clogged.
What Are The Warning Signs And Symptoms Of A
Stroke?
Warning signs and symptoms of stroke include: sudden weakness or numbness of
the face, arm or leg; sudden dimness or loss of vision, particularly in one
eye; sudden difficulty speaking or understanding speech; sudden severe headache
with no known cause; and unexplained dizziness, unsteadiness, or sudden falls,
especially with any of the other signs. Warning signs may last a few moments
and then disappear. When they disappear within 24 hours or less, they are
called a transient ischemic attacks (TIA). Attack: Stroke
Warning Signs and Risk Factors and Brain Basics:
Preventing Stroke.
Warning Signs Of A Stroke
If you observe one or more of these signs of a stroke or "brain
attack," don't wait, call a doctor or 911 right away!
Sudden weakness or numbness of the face, arm, or leg on one
side of the body.
Sudden dimness or loss of vision, particularly in one eye.
Sudden difficulty speaking or trouble understanding speech.
Sudden severe headache with no known cause.
Unexplained dizziness, unsteadiness, or sudden falls,
especially with any of the other signs.
Warning signs may last a few moments and then disappear. They
are signs of a serious condition that won't go away without medical help.
Risk Factors For A Stroke
Stroke prevention is still the best medicine. The most
important treatable conditions linked to stroke are:
High blood pressure. Eat a balanced diet, maintain a healthy
weight, and exercise to reduce blood pressure. Drugs are also available.
Cigarette smoking. Medical help is available to help quit.
Heart disease. Your doctor will treat your heart disease and
may also prescribe medication to help prevent the formation of clots. If you
are over 50, NINDS scientists believe you and your doctor should make a
decision about aspirin therapy.
Diabetes. Treatment can delay
complications that increase the risk of stroke.
Transient
ischemic attacks. These are brief episodes of stroke's warning signs and can be
treated with drugs or surgery.
How Important Is A Blockage As A Cause Of
Stroke?
A blockage of a blood vessel is the most frequent cause of stroke and is
responsible for about 75 percent of the nearly 150,000 U.S. stroke deaths each
year. Stroke ranks as the third leading killer in the United States after heart
disease and cancer. There are 500,000 to 600,000 new strokes in the United
States each year. As many as 3 million Americans have survived a stroke with
more than 2 million of them sustaining some permanent disability. The overall
cost of stroke to the nation is $30 billion a year.
How Many Carotid Endarterectomies Are Performed
Each Year?
In 1992, the most recent year for which statistics are available from the
National Hospital Discharge Survey, there were about 91,000 carotid
endarterectomies performed in the United States. The procedure has a 40-year
history. It was first described in the mid-1950s. It began to be used
increasingly as a stroke prevention measure in the 1960s and 1970s. Its use
peaked in the mid-1980s when more than 100,000 operations were performed each
year. At that time, several authorities began to question the trend and the
risk-benefit ratio for some groups, and the use of the procedure dropped
precipitously. The NINDS-supported North American Symptomatic Carotid
Endarterectomy Trial (NASCET) and the NINDS-supported Asymptomatic Carotid
Atherosclerosis Study (ACAS) were launched in the mid-1980s to identify the
specific groups of people with carotid artery disease who would clearly benefit
from the procedure. Dr. Szarnicki was a principal surgical investigator in both NASCET and ACAS studies. He performs this operation 2-5 times per month or more on ocassion.
How Much Does A Carotid Endarterectomy Cost?
The total average cost for the diagnostic tests, surgical procedure,
hospitalization, and follow up care is about $15,000. Most, if not all is covered by insurance.
How Risky Is The Surgery?
The degree of risk varies with the hospital, the surgeon, and the underlying
disease conditions. The risk of stroke is 1-3% in the hands of a skilled surgeon. Patients with cardiac disease need careful preoperative evaluation to reduce the risk of a heart attack.
How Is Carotid Artery Disease
Diagnosed?
In most cases, the disease can be detected during a normal checkup with a
physician. Some of the tests a physician can use or order include history and
physical exam, doppler ultrasound imaging, oculoplethysmography (OPG), computed
tomography (CT), arteriography and digital subtraction angiography (DSA),
magnetic resonance angiography (MRA). Frequently these procedures are carried
out in a stepwise fashion: from a doctor's evaluation of signs and symptoms to
ultrasound, with arteriography, DSA or MRA reserved for difficult diagnoses.
History and physical exam. A doctor will ask about symptoms of
a stroke such as numbness or muscle weakness, speech or vision difficulties, or
lightheadedness. Using a stethoscope, a doctor may hear a rushing sound, called
a bruit (pronounced "brew-ee"), in the carotid artery. Unfortunately, dangerous
levels of disease sometimes fail to make a sound, and some blockages with a low
risk can make a sound.
Doppler ultrasound imaging. This is a painless, noninvasive
test in which sound waves above the range of human hearing are sent into the
neck. Echoes bounce off the moving blood and the tissue in the artery and can
be formed into an image. Ultrasound is fast, risk-free, relatively inexpensive
and painless. Unfortunately, there is a small possibility of error in an
ultrasound study. A stenosis with a high level of risk will occasionally be
incorrectly reported as a low-risk finding. Conversely, a stenosis with a low
level of risk will sometimes be reported as a high level of risk. In carefully
calibrated ultrasound laboratories, ultrasound studies can be up to 95 percent
accurate and offer visualization of the anatomy, evaluation of the blood flow
rate and turbulence, and characterization of the plaque. Performing an
ultrasound study requires a great deal of skill which is not always available.
Oculoplethysmography (OPG). This procedure measures the
pulsation of the arteries in the back of the eye. It is used as an indirect
check for blockages in the carotid arteries.
Computed Tomography (CT). This test produces a series of
cross-sectional X-rays of the head and brain. It cannot detect carotid artery
disease but may be ordered by a doctor to investigate other possible causes of
symptoms. The test is also called a CAT scan, for computer assisted tomography.
Arteriography and Digital Subtraction Angiography (DSA).
Arteriography is an X-ray of the carotid artery taken when a small flexible
catheter is threaded up the aorta into the Common Carotid Artery (right or
left) and then a special dye is injected which gives the physician a roadmap of
the Internal and External Carotid arteries. A warm sensation may be felt when
the dye is injected. DSA is also an X-ray study of the carotid artery. It is
similar to conventional arteriography except that less dye is used. A person
having a DSA must remain still during the test. These invasive procedures are
more expensive and carry their own small risk of causing a stroke.
Magnetic Resonance Angiography (MRA). This is a very new
imaging technique that is more accurate than ultrasound yet avoids the risks
associated with X-rays and dye injection. An MRA is a type of magnetic
resonance image that uses special software to create an image of the arteries
in the brain. A magnetic resonance image uses harmless but powerful magnetic
fields to create a highly detailed image of the body's tissues.
Please note, Arteriograpy and or MRA are only done when Ultrasound doesn't provide sufficient detail to carefully plan surgery.
What Is "Best Medical Therapy" For Stroke
Prevention?
The mainstay of stroke prevention is risk factor management: smoking cessation,
treatment of high blood pressure and heart disease, and control of blood sugar
levels among persons with diabetes. Additionally, physicians may prescribe
aspirin, warfarin, or ticlopidine. See also Brain Basics:
Preventing Stroke. In addition, here is a link to the latest information
from the American Heart Association regarding Guidelines
for Carotid Endarterectomy.
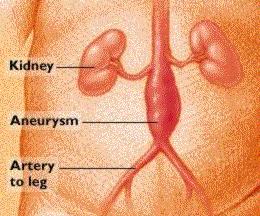
An aneurysm is a bulging or ballooning of an artery wall. It usually occurs
when the arterial wall becomes weak or damaged by accumulation of
cholesterol-containing fatty deposits (atherosclerosis).
Other factors that contribute to weakening of the arterial wall are:
High blood pressure
Smoking
Male gender
Age 55 or older
Family history of abdominal aortic aneurysm.
Once elasticity is reduced, the force of the heartbeat can cause an artery to
slowly stretch and bulge.
An abdominal aortic aneurysm occurs in your body's largest artery, the aorta.
Usually, this aneurysm develops beyond where the aorta branches to supply blood
to your kidneys and above where it divides to supply blood to your pelvis and
legs.
The abdominal aorta's diameter normally ranges from 3/4 to 1 inch. Small
aneurysms--less than 2 inches (5 centimeters)--rarely rupture. As they grow
bigger than this, however, the risk of rupture increases by 5 percent each
year.
As with any aneurysm, the danger is that an abdominal aortic aneurysm will leak
or burst, causing life-threatening bleeding. A few people may feel pain in
their backs as an aneurysm enlarges. But most abdominal aortic aneurysms are
"silent" they enlarge slowly with no symptoms.
If you're at high risk:
A careful physical examination can detect 70 to 80 percent of abdominal aortic
aneurysms. By placing a stethoscope on your abdomen, your doctor can pick up
sounds of turbulent blood flow over the aorta's roughened surface. Gentle
pressure on your abdomen can help determine whether you have a pulsating
mass.
Being overweight, however, reduces accuracy. And, usually, further evaluation
is needed. For a more accurate test, your doctor may use ultrasound.
Routine screening for an aortic aneurysm using computed tomography (CT) or
magnetic resonance imaging (MRI) scans isn't usually necessary or
cost-effective.
When do you need surgery?
Surgery is almost always needed when the diameter of an aneurysm enlarges to at
least 2 inches. The operation involves an incision into your abdomen to open
the aorta and remove cholesterol and fatty buildup. The surgeon implants a
flexible tube (graft) to replace the enlarged artery. Recovery from elective
surgery takes about six weeks, including a one-week hospital stay.
Emergency repair of a ruptured aortic aneurysm is less successful--62 percent
of people die before they reach the hospital. Of those who have surgery, 50
percent live.
As an alternative to abdominal surgery, Mayo Clinic is one of several medical
centers investigating a new procedure called endovascular surgery. It involves
passing a collapsed graft up the femoral artery in your leg into the weakened
aorta, then securing the graft with metallic stents. Similar to balloon
angioplasty, the graft is then inflated to restore normal blood flow.
Endovascular surgery may become a safer and easier alternative to traditional
surgery, especially for people at high surgical risk.
Find out sooner, not later
Prevention and early detection are the keys to avoiding death from an abdominal
aortic aneurysm. If you're at least 55 years old, know your risks and what
steps you can take to protect yourself.
Patients with arteriosclerosis obliterans have symptoms related to the slow,
insidious development of tissue ischemia. The initial symptom is
intermittent claudication, a deficient blood supply in exercising
muscle. The distress is described as a pain, ache, cramp, or tired feeling that
occurs on walking; it occurs most commonly in the calf but also in the foot,
thigh, hip, or buttocks. Symptoms are relieved quickly by rest (usually in 1 to
5 min), and the patient can walk as far again before pain recurs. Sitting is
not necessary to obtain relief. Distress is worsened by walking rapidly or
uphill but, by definition, claudication never occurs at rest. Progression of
the disease is indicated when the distance that the patient can walk is
diminishing. Similar symptoms related to exertion can occur with involvement of
the upper extremity.
The occlusive disease may progress so that ischemic pain occurs at rest. Rest
pain beginning in the most distal parts of a limb is a severe, unrelenting pain
aggravated by elevation and often preventing sleep; for relief, the patient
will hang his foot over the bedside or will rest in a chair with legs
dependent.
If intermittent claudication is the only symptom, the extremity may appear
normal, but the pulses are reduced or absent. The level of arterial occlusion
and the location of intermittent claudication are closely correlated; eg,
aortoiliac disease frequently causes claudication in the buttocks, hips and
calves, and the femoral pulses are absent; in males, impotence is common and
depends on the location and extent of occlusion. In femoropopliteal disease,
claudication is typically in the calf, and all pulses below the femoral are
absent. In patients with small vessel disease (eg, Buerger's disease or
diabetes mellitus), the femoral and popliteal pulses are present but foot
pulses are absent. Helpful confirmatory signs of arterial insufficiency are
pallor of the involved foot after 1 to 2 min of elevation, followed by redness on
dependency. Venous filling time on dependency following elevation is delayed
beyond the normal limit of 15 sec. If claudication occurs in the presence of
good distal pulses, spinal stenosis should be considered as part of the
differential diagnosis.
A severely ischemic foot is painful, cold, and often numb. The skin may be dry
and scaly with poor nail and hair growth. As ischemia worsens, ulceration may
appear, especially after local trauma, typically on the toes or heel or
occasionally on the leg. There is usually no edema, but a severely ischemic leg
may be shrunken and atrophic.
More extensive obliterative disease may compromise the viability of tissues and
lead to necrosis or gangrene.
Acute ischemia is caused by sudden arterial occlusion by embolization from the
heart, a proximal arteriosclerotic plaque, or an aneurysm, or by an acute
thrombosis on preexisting atherosclerotic disease. The history includes sudden
onset of severe pain, coldness, numbness, and pallor. The extremity is cold,
either pale or cyanotic, and pulses are absent distal to the obstruction. In
acute occlusion of the aorta (saddle embolus or thrombosis), all pulses in the
lower extremities are absent. Typically, acute occlusions occur at bifurcations
just distal to the last palpable pulse; thus, with occlusion at the common
femoral bifurcation, the femoral pulse is palpable, and with occlusion at the
popliteal bifurcation, the popliteal pulse is present. Acute occlusion may
cause severe ischemia manifested by sensory and motor loss and induration of
muscles on palpation.
Treatment Options:
Patients with intermittent claudication should walk 60 min/day, if possible;
when discomfort occurs, they should stop, allow the pain to disappear, and then
walk again. This mode of treatment will significantly improve the distance a
patient can walk without discomfort; the mechanism is not precisely known but
could be the result of both physical training and an increase in collateral
circulation as a result of muscle demand. Tobacco in all forms must be
eliminated. Vasodilators are commonly prescribed, although there is no proof of
their effectiveness. beta-Blocking agents may worsen intermittent claudication;
this effect should be anticipated in these patients. When a patient is
sleeping, blocks should be used to elevate the head of the bed 4 to 6 in.
Pentoxifylline 400 mg tid may improve intermittent claudication in selected
cases, by improving blood flow and enhancing tissue oxygenation in affected
areas. Recent studies seem to indicate that calcium antagonists and thromboxane
inhibitors may be clinically useful in managing patients with both occlusive
and vasospastic arterial diseases. Chelation therapy has no proven role and is
not recommended.
Prophylactic foot care is especially important: (1) Patients should inspect and
feel their feet daily for cracks, fissures, calluses, corns, and ulcers. (2)
Feet should be washed daily in lukewarm water, using mild soap; they should be
dried gently and thoroughly. (3) A lubricant, such as lanolin, should be used
for dry, scaly skin. (4) Bland, nonmedicated foot powders should be used for
moist feet. (5) Toenails should be cut straight across, not too close to the
skin. A podiatrist should do this if the patient's eyesight is poor. (6)
Calluses or corns should be treated by a podiatrist. (7) Adhesive plasters and
tape should not be used on skin. (8) Harsh chemicals or corn cures should not
be used. (9) Patients should change stockings daily and avoid constricting
garters. (10) Loose wool stockings can keep feet warm in cold weather, but hot
water bottles or electric pads must not be used. (11) Shoes should fit well;
they should be wide-toed without open heels or toes and should be changed
frequently. (12) Special shoes should be prescribed if there is any foot
deformity (eg, previous toe amputation, hammer toe, bunion) in order to reduce
trauma. (13) Walking barefoot should always be avoided.
In patients with diabetic neuropathic ulcers, weight bearing should be avoided
or, if this is not possible, appropriate orthotic protection of the ulcer
should be used. Since most patients with this type of ulcer have little or no
macrovascular occlusive disease, debridement, trimming of callus, and
antibiotic administration frequently produce good healing. Drainage of
infection may prevent major surgery later. After the ulcer has healed,
appropriate inserts or special shoes should be prescribed. Refractory cases,
especially if osteomyelitis is present, may require surgical removal of the
metatarsal head (source of pressure), combined with amputation of the involved
toe or a transmetatarsal amputation. A neuropathic joint may be satisfactorily
managed with orthopedic appliances such as short leg braces, molded shoes,
sponge-rubber arch supports, crutches, and prostheses.
In ischemic foot lesions, if revascularization is impossible, a therapeutic
program may prevent amputation. Diabetes mellitus must be controlled as closely
as possible, and complete bed rest with the head of the bed elevated on blocks
is necessary. The lesion must be kept clean with daily soaks in mild soap or
NaCl solution and then dressed with sterile dry dressings. A mild antibiotic
ointment may be used. Irritating and sensitizing solutions should be avoided.
Obvious infection should be cultured and appropriate antibiotics given
systemically. Enzymatic debridement may be irritating and increase the pain.
Surgical debridement when ischemia is severe does more harm than good and is
very painful. Patients should be warned that healing may take a long
time.
Percutaneous transluminal angioplasty (PTA) has proved useful for the treatment
of localized occlusive arterial lesions due to atherosclerosis. With
appropriate patient selection, which depends upon complete, adequate
angiography, the success rate approaches 95% in the iliac arteries and 50 to
60% in the thigh and calf arteries. When PTA is successful, the results are
gratifying, a surgical procedure is avoided, and only 1 or 2 days of
hospitalization are required. Surgical backup should always be available. The
technique, usually done by a radiologist or cardiologist, consists of dilating
the diseased segment with the Gr�ntzig double lumen catheter, containing a
balloon made of noncompliant high-pressure plastics (eg, polyethylene
terephthalates [PET], polyvinyl chloride [PVC]). It can be inflated up to 12
atmospheres pressure while maintaining a cylindrical balloon shape. A
postdilation arteriogram or digital subtraction angiogram is usually done
during the procedure. The small size of the flexible catheters allows various
approaches to many arteries, such as renal, other visceral, coronary, axillary,
iliac, and superficial femoral-popliteal arteries. The procedure is not painful
but may be somewhat uncomfortable from lying on an x-ray table. Mild sedation,
but not general anesthesia, is used. Following dilation, to prevent reocclusion
by thrombosis, the patient may be given heparin in the usual doses IV for 24
hours. Many physicians prefer to give their patients aspirin or another
antiplatelet agent. Noninvasive studies (see above) should be done before and
after the dilation to document improvement and to follow up the
patient.
Indications for PTA of peripheral arteries are similar to those for surgery:
(1) progressive and limiting intermittent claudication that prevents the
patient from working, (2) rest pain, and (3) gangrene. Various reports document
success for optimal lesions as >= 90%. Suitable lesions are flow-limiting,
short iliac stenoses and short, single or multiple stenoses of the superficial
femoral-popliteal segment. Complete occlusions of the superficial femoral
artery, < 10 to 12 cm, have been successfully dilated, but better success
results if lesions are < 5 cm. An excellent indication for PTA is a short
localized iliac stenosis prior to a distal femoropopliteal bypass operation.
The decision to perform PTA should be made jointly by a vascular surgeon,
radiologist, and/or cardiologist.
Contraindications are diffuse disease, long occlusions, and severe arterial
calcification. Complications that may require surgical intervention are
thrombosis at the site of dilation, distal embolization, intimal dissection
with occlusion by a flap, and those from heparin therapy.
New devices, in addition to balloons, now include lasers, mechanical cutters,
ultrasonic catheters, stents, and rotational sanders. No one type of device has
been proved superior to another, and choice is best made by the physician
performing the procedure.
Reconstructive surgical procedures are well established and valuable. In
properly selected patients, symptoms are relieved, ulcers healed, and
amputations averted. The procedures are thromboendarterectomy, bypass graft
(woven prosthetic tube or autogenous vein anastomosed end-to-side to the vessel
above and below the obstruction), or resection with graft replacement (most
often used in cases of abdominal aortic aneurysm and proximal atheromatous
arteries that embolize peripherally). Effective surgery depends on adequate
angiography (aortography and bilateral femoral arteriography) that establishes
the site of occlusion and the condition of the arteries above and
below.
Success of a surgical procedure is directly related to the adequacy of blood
flow into (run in) and out of (run off) the graft. Autogenous veins (usually
the greater saphenous) are used most often to bypass occlusive lesions of the
superficial femoral, popliteal, or tibial arteries. Thromboendarterectomy is
used for short localized lesions in the aorta, iliac, common femoral, or deep
femoral arteries. Woven Dacron is the preferred material for an arterial
prosthesis to bypass disease in the aortoiliac area. PTFE (Gore-Tex®) is
the synthetic of choice for femoropopliteal-tibial obstructions, if saphenous
vein is not available. The indications for surgical procedures in the
aortoiliac area are incapacitating (economic or avocational) intermittent
claudication or severe ischemia due to associated distal disease. Surgery for
femoropopliteal and/or tibial disease is reserved for patients who have severe
ischemia with rest pain, ulceration, or minor gangrene. Patients with only
intermittent claudication should always be treated conservatively at first; if
the disease progresses to more severe ischemia, surgery is needed. In some
cases, sympathectomy, which removes neurogenic vasoconstriction, can be very
helpful and should be offered to selected patients with severe disease and
those who are not candidates for revascularization. The value of
revascularization procedures is well established in terms of limb salvage and
relieving claudication, but reduction in mortality is small.
When amputation is required for uncontrolled infection, unrelenting rest pain,
and progressive gangrene, it should be kept as distal as possible; it is
especially important to preserve the knee for optimal use of a prosthesis.